
1 out of 10 women have endometriosis, a condition that can significantly impact a person’s quality of life. As with many conditions, the earlier the diagnosis, the better the treatment outcomes. Unfortunately, laparoscopy, an invasive procedure, is currently the only definitive way to diagnose endometriosis.
What Is Endometriosis?
If you are facing a diagnostic laparoscopy due to your endometriosis-related symptoms, you may be eligible to participate in the EndoCheck clinical trial.
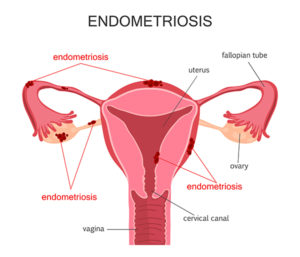
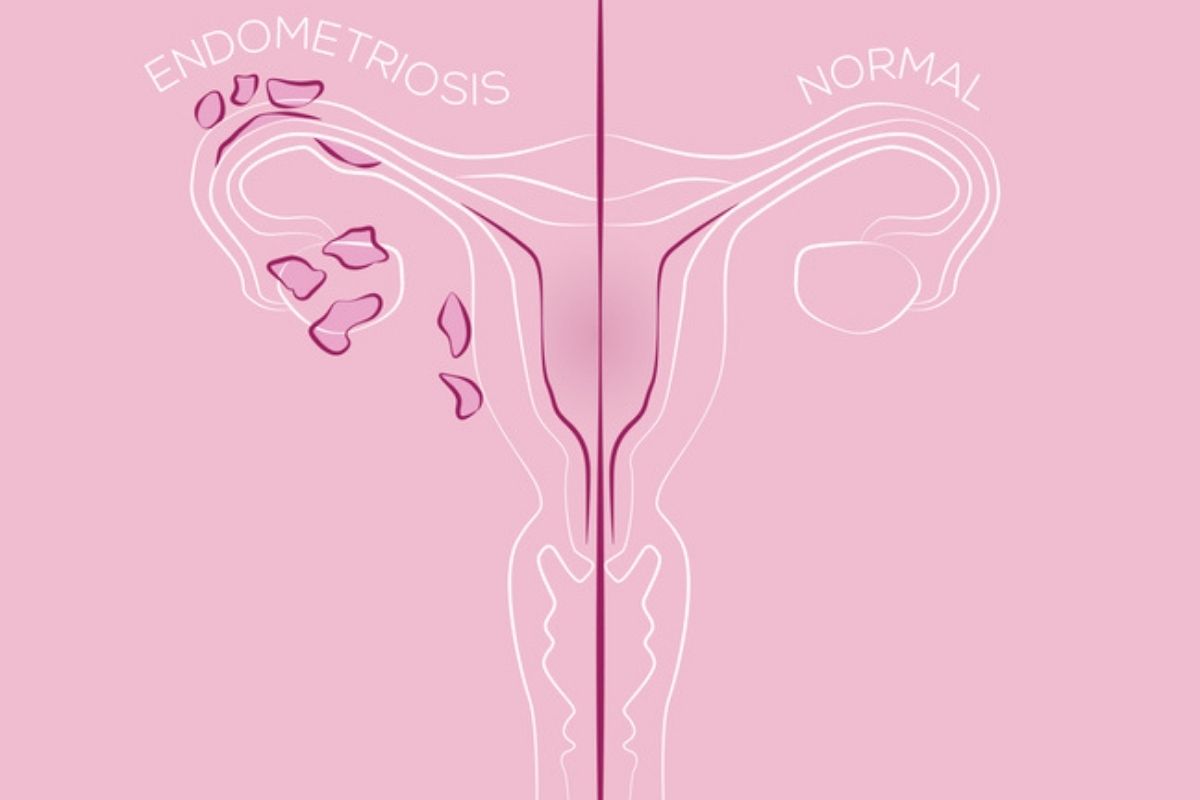
Endometriosis is a chronic medical condition in which tissue similar to the lining of the uterus, called the endometrium, grows outside the uterus. Normally, the endometrium remains within the uterus and simply thickens throughout the month before being shed during menstruation. With endometriosis, this tissue grows in the pelvic cavity, on the surface of the uterus, and other organs, such as the ovaries, fallopian tubes, and tissues lining the pelvis.
While the endometrium is shed during menstruation and exits via the vaginal opening, the tissue outside of the uterus has no way to leave the body. Over time, this can cause inflammation, scarring, and painful adhesions.
Stages of Endometriosis
Endometriosis is classified into stages based on the severity, extent, and location of the disease.

The staging system used to classify endometriosis is the Revised American Society for Reproductive Medicine (rASRM), which categorizes endometriosis into four stages.
- Stage 1 endometriosis is considered minimal, typically with minimal adhesions or scar tissue, and generally localized within the pelvic cavity.
- Stage 2 endometriosis is mild, with numerous or slightly larger lesions, and involves both ovaries and other pelvic structures.
- Stage 3 endometriosis is moderate, with multiple implants or lesions and deeper infiltrating lesions affecting the ovaries, fallopian tubes, or uterus. It may distort the anatomy and organ function.
- Stage 4 endometriosis is severe and consists of extensive implants or lesions scattered throughout the pelvic cavity. It may extend to other parts of the body, such as the bowels or bladder.
Endometriosis at a more advanced stage does not always mean you will have more severe symptoms or pain. For example, some women with stage 4 endometriosis may have few or no symptoms, whereas others with stage 1 can experience severe symptoms.
Endometriosis Evaluation and Diagnosis
In order to diagnose endometriosis, a doctor will assess medical history, perform a pelvic exam, and run diagnostic tests.
During the review of your medical history, your doctor will ask about your symptoms, whether you have any risk factors associated with endometriosis, your periods and pelvic pain, and whether you are experiencing infertility.

During the pelvic exam, your doctor will check for tenderness or pain. Afterward, your doctor may order imaging tests to examine the tissues around your pelvic area visually. Your doctor may make a “clinical diagnosis,” but this is not currently definitive without an invasive laparoscopy procedure.
A laparoscopy involves a small incision made in the abdomen near the belly button. The surgeon will insert a laparoscope – a long, thin tube equipped with a light and camera – through the incision before inflating the abdominal cavity with carbon dioxide gas. This will allow the surgeon to identify and examine any endometrial implants and even take a biopsy to send for laboratory analysis.
While laparoscopies are far less invasive than open-cavity surgery, they still involve some risk and recovery time. Fortunately, research is ongoing to demonstrate the effectiveness of a new diagnostic tool, the EndoCheck clinical test.
What Is EndoCheck?
If you are scheduled to undergo diagnostic laparoscopy to be evaluated for endometriosis, you may be eligible to access a non-invasive blood test called EndoCheck. This diagnostic test for endometriosis can help your gynecological professional diagnose endometriosis and guide decisions related to your ongoing care. Help us as we work to validate this procedure, potentially eliminating the need for laparoscopy in the future.
To be eligible to participate, you must:
- Be able to provide written and informed consent or obtain the consent of an authorized representative or guardian.
- Be a female aged 14 to 50 years old.
- Be scheduled to undergo laparotomy or laparoscopy for suspected endometriosis.
How the EndoScope Clinical Trial Works
If you choose to participate, the endometriosis clinical trial will last approximately three months and include two visits to the Arizona Gynecology Consultants office. Upon arrival, you will complete an informed consent form along with an Endometriosis Health Profile Questionnaire and case report forms. Afterward, a blood sample will be collected.

After your laparoscopy, and if you are confirmed to have endometriosis, you will complete the Endometriosis Health Profile Questionnaire again. We will compare the results of the blood study test to the pathology reports and surgical observations obtained during your surgery.
Why Participate?
The goal of EndoCheck is to evaluate a new investigational test that may be able to detect endometriosis without the invasive procedure. Participating in this study allows you to be a part of changing the endometriosis prognosis journey and improving women’s quality of life. It may also reveal additional information about the medical roots of endometriosis.
Endometriosis Causes
The exact cause of endometriosis is not clear, but researchers have identified some promising theories.
Retrograde Menstruation
One theory suggests that during menstruation, some of the menstrual blood containing endometrial cells flows backward through the fallopian tubes into the pelvic cavity instead of leaving the body. These cells then implant and grow on the pelvic organs, causing endometriosis.
Coelomic Metaplasia
The theory of coelomic metaplasia suggests that certain cells lining the pelvic cavity can transform into endometrial-like tissue in response to hormonal or inflammatory signals. These transformed cells then create endometriosis lesions.
Embryonic Cell Changes
Some researchers speculate that endometriosis may result from embryonic cells that retain the ability to develop into various types of tissue, including endometrial-like tissue. These cells may become misplaced during embryonic development and create endometriosis lesions later in life.
Surgical Scar Complication
Surgical procedures involving the reproductive organs or pelvic cavity can cause tissue trauma, inflammation, and scarring, which may create an environment prime for the development of endometriosis. Inflammatory processes associated with surgical healing can promote the adhesion and proliferation of endometrial cells outside of the uterus.
Immune System Condition
A potential problem with the immune system is that the body may not recognize and destroy endometriosis tissue since it is produced within the body. Endometriosis has also been associated with systemic lupus erythematosus (SLE) and Hashimoto’s thyroiditis.
Genetics
Endometriosis may affect some people more often due to a genetic trait passed down in their families. Women with a close relative who has endometriosis, such as a mother, sister, or daughter, are at an increased risk of developing the condition themselves compared to those with no family history.
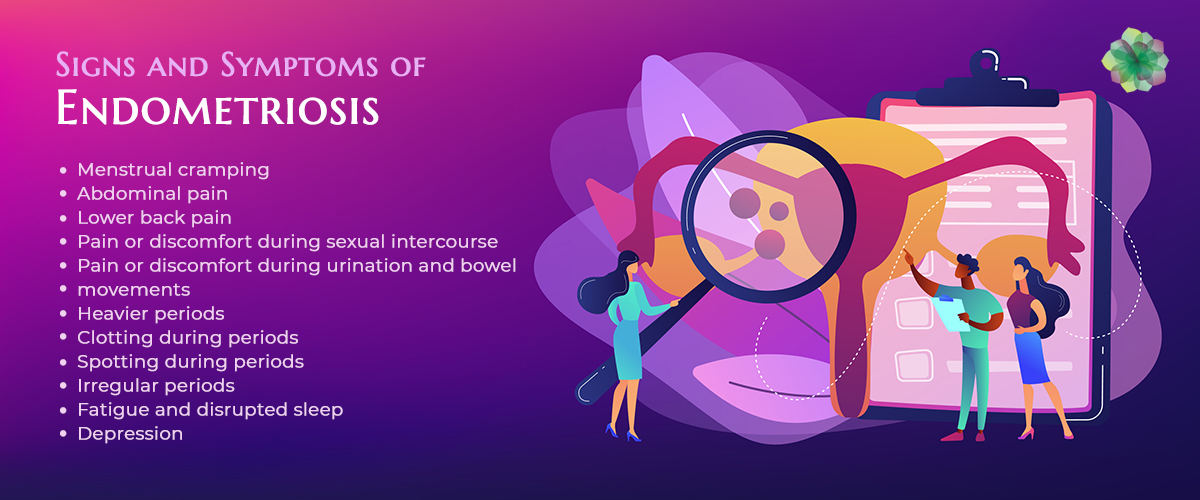
Endometriosis Symptoms
The main symptom of endometriosis is pelvic pain, often linked with menstruation. This pain can be a dull ache, cramping, or even sharp stabbing sensations, depending on the person. It may even worsen over time.
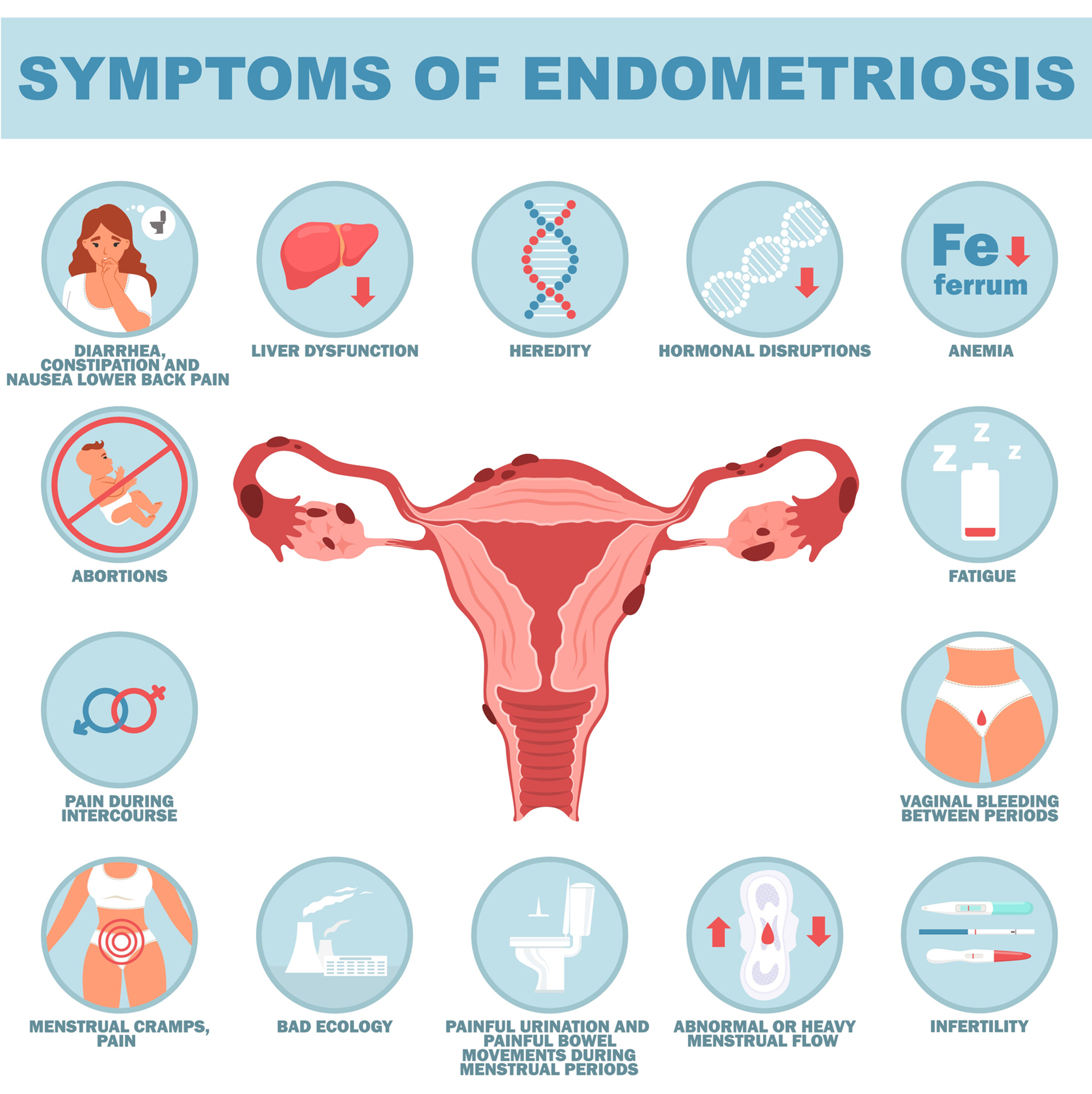
Other common symptoms include:
Painful Periods
Painful periods, medically known as dysmenorrhea, are a common symptom of endometriosis. This pain can be debilitating and may interfere with daily activities and quality of life. Some people with endometriosis experience deep pelvic pain or pressure during menstruation from the presence of endometrial implants or lesions near the cervix, uterus, ovaries, or rectum. Endometriosis pain can also impact the lower back, thighs, or buttocks.
Dyspareunia
Dyspareunia occurs when endometrial or scar tissue in the pelvic region causes pain or discomfort during sexual intercourse. This can lead to difficulties with intimacy and potential strain on relationships.
Infertility
Endometriosis is the leading cause of infertility in women, affecting up to 30-50% of women who experience infertility. The disease can distort pelvic anatomy, interfere with ovulation, and damage eggs and sperm. Alterations in the endometrial lining may also affect embryo implantation and early pregnancy development, along with changes in hormone levels, inflammation, and immune system dysfunction.
Gastrointestinal Symptoms
Endometrial growths on pelvic organs and bowels can lead to bloating, constipation, diarrhea, abdominal cramping, and nausea and vomiting. Endometrial growths or adhesions near the rectum or sigmoid colon can cause discomfort or pain during bowel movements. These can all worsen during menstruation.
Fatigue
Chronic pain and discomfort, pain management, coping with symptoms, and disrupted sleep patterns can contribute to fatigue and exhaustion. This is an often overlooked symptom, but it can significantly impact a person’s quality of life.
Urinary Symptoms
Some women may experience endometrial growths that affect the urinary tract. Endometriosis can cause interstitial cystitis (IC), which is a chronic condition that causes bladder pain, urinary urgency, frequency, and discomfort. Women with endometriosis may also be at an increased risk of urinary tract infections because of urinary retention, inflammation, or obstruction caused by endometrial growths or adhesions.
Other Symptoms
Endometriosis can also cause back pain, leg pain, heavy menstrual bleeding, and irregular menstrual cycles. The extent and severity of these symptoms will vary among each individual, and some women do not have any symptoms. As mentioned, having a more advanced stage of endometriosis, such as stage 4, does not mean more severe symptoms or pain.
Many symptoms may not be typically associated with endometriosis, which can complicate diagnosis and treatment. People may think they have irritable bowel syndrome (IBS) or uterine fibroids, but diagnostics reveal endometriosis.
Treatment Options
While endometriosis currently has no cure, there are treatment options available to help manage pain, slow tissue and implant growth, and help with potential infertility.
The first line of treatment is medication, such as nonsteroidal anti-inflammatory drugs (NSAIDs) and acetaminophen, combined (estrogen-progestin) contraceptives, progestin, gonadotrophin-releasing hormone (GnRH) agonists, danazol, or aromatase inhibitors are the most commonly prescribed.
If medications are not working, surgery may be a choice. Surgeries may be used to remove scar tissue and endometrial implants or hysterectomy with or without bilateral scalping-oophorectomy. This involves the removal of the uterus while leaving or removing the ovaries and fallopian tubes.
What are the Risk Factors for Endometriosis?
It is possible to develop endometriosis later in life, but it usually manifests during a woman’s reproductive years.

Factors that raise the risk of endometriosis include:
- Starting your period at an early age
- Starting menopause at an older age
- An abnormal uterus
- Heavy periods that are longer than seven days
- A menstrual cycle that is shorter than 27 days
- Higher levels of estrogen in your body or greater exposure to estrogen than your body normally produces
- Low body mass index
- You have a genetic connection to family members with endometriosis.
Additionally, any health condition that prevents menstrual blood from leaving your body can increase your risk of endometriosis.
Help Reduce the Impact of Endometriosis
Endometriosis can significantly impact a woman’s life, including physical health, emotional well-being, relationships, work, and social activities, due to severe pain, fatigue, infertility, anxiety, and depression. Addressing endometriosis will help empower those experiencing it and improve women’s sexual and reproductive health, quality of life, and well-being. First, however, it’s crucial to make the process of diagnosing endometriosis as painless and stress-free as possible. We urge you to consider participating in the EndoCheck clinical trial and potentially help minimize the impact of endometriosis on others.
If you’re interested, please contact your surgeon at Arizona Gynecology Consultants for further information.
Resources:
- Endometriosis. (2021, February). Www.acog.org. https://www.acog.org/womens-health/faqs/endometriosis
- World Health Organization. (2023, March 24). Endometriosis. World Health Organization; World Health Organization. https://www.who.int/news-room/fact-sheets/detail/endometriosis
- Matsuura, K., Ohtake, H., Katabuchi, H., & Okamura, H. (1999). Coelomic metaplasia theory of endometriosis: evidence from in vivo studies and an in vitro experimental model. Gynecologic and Obstetric Investigation, 47 Suppl 1, 18–20; discussion 20-2. https://doi.org/10.1159/000052855
- John Hopkins Medicine. (2024). Endometriosis. John Hopkins Medicine. https://www.hopkinsmedicine.org/health/conditions-and-diseases/endometriosis
- Endometriosis. (n.d.). Yale Medicine. https://www.yalemedicine.org/conditions/endometriosis
- Mayo Clinic. (2023, October 12). Endometriosis – Symptoms and Causes. Mayo Clinic. https://www.mayoclinic.org/diseases-conditions/endometriosis/symptoms-causes/syc-20354656
- Bafort, C., Beebeejaun, Y., Tomassetti, C., Bosteels, J., & Duffy, J. M. (2020). Laparoscopic surgery for endometriosis. Cochrane Database of Systematic Reviews, 10(10). https://doi.org/10.1002/14651858.cd011031.pub3
- Endometriosis: Does It Cause Infertility? (n.d.). Www.reproductivefacts.org. https://www.reproductivefacts.org/news-and-publications/fact-sheets-and-infographics/endometriosis-does-it-cause-infertility/
- American Society for Reproductive. (1997). Revised American Society for Reproductive Medicine classification of endometriosis: 1996. Fertility and Sterility, 67(5), 817–821. https://doi.org/10.1016/s0015-0282(97)81391-x

Dr. Waliser is a gynecology specialist, performs minimally invasive surgery, and has been practicing medicine for over 22 years, primarily in the Scottsdale and Tucson areas. He graduated from the University of North Dakota School of Medicine & Health Sciences and completed his residency at St. Francis Hospital. Dr. Waliser is fellowship trained in Advanced Laparoscopy/Hysteroscopy and is board certified.









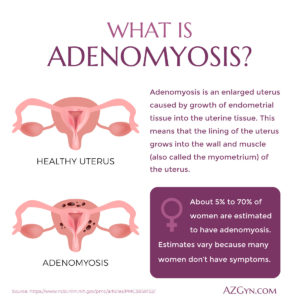 Adenomyosis is a condition in which the endometrium, instead of growing out into the uterus, grows into the uterine wall (myometrium). Each time the lining (endometrium) is stimulated, during the menstrual cycle, the trapped lining in the myometrium is also stimulated and can make menstrual cramps and pain worse. This can disrupt the quality of life for the women who have to deal with it. And because adenomyosis symptoms vary due to he flux of estrogen levels going up and down, the menstrual cycle brings more discomfort than usual.
Adenomyosis is a condition in which the endometrium, instead of growing out into the uterus, grows into the uterine wall (myometrium). Each time the lining (endometrium) is stimulated, during the menstrual cycle, the trapped lining in the myometrium is also stimulated and can make menstrual cramps and pain worse. This can disrupt the quality of life for the women who have to deal with it. And because adenomyosis symptoms vary due to he flux of estrogen levels going up and down, the menstrual cycle brings more discomfort than usual.
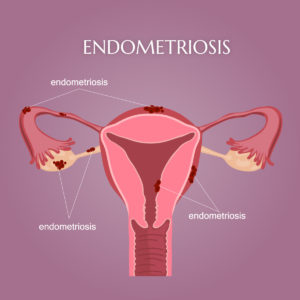 Endometriosis is a complex condition that often results in serious and painful symptoms. Endometrium typically grows on the interior of the uterine walls and thickens, breaks down, and then bleeds with each menstrual cycle. When endometrium forms on the outside of the uterine walls, it can affect the ovaries, fallopian tubes, and other pelvic organs in rare cases.
Endometriosis is a complex condition that often results in serious and painful symptoms. Endometrium typically grows on the interior of the uterine walls and thickens, breaks down, and then bleeds with each menstrual cycle. When endometrium forms on the outside of the uterine walls, it can affect the ovaries, fallopian tubes, and other pelvic organs in rare cases.